|
Prostate-Cancer Gene
Test Helps Patients Decide on Treatment
WSJ | Health By Lucette Lagnado, March 31, 2018 https://www.wsj.com/articles/prostate-cancer-gene-test-helps-patients-decide-on-treatment-1522494300
In 37 years as a police officer, Edwin Michel coped with a plane crash, a sniper, wildfires and three bullet wounds. Nothing much rattled him until he was diagnosed with prostate cancer in November 2016. His doctor said the cancer wouldn't kill him but Mr. Michel, now 76 years old, wasn't entirely reassured. He felt more confident after a genomics test later revealed his prostate cancer was very low risk. The test, known as Oncotype DX, takes a sample from a prostate biopsy and analyzes 17 genes in it to estimate how aggressive a cancer may be. Mr. Michel, who retired as chief of patrol for Suffolk County, N.Y., didn't have surgery to remove the cancer. Instead he went on "active surveillance," where the disease is closely monitored. His doctor, Aaron Katz, chairman of urology at NYU Winthrop Hospital in Mineola, N.Y., recommends active surveillance when possible. He says he wants to spare men the side effects that can happen if a cancerous prostate is removed or radiated. For Dr. Katz, the genomics test "is an extremely important diagnostic tool to help me identify patients who are best to go on to surveillance." In the U.S., there are 165,000 new cases of prostate cancer a year and about 29,000 deaths from the disease. Researchers say some men with low-risk prostate cancer, which may not require intervention, have been overtreated. Improved treatments mean men with prostate cancer are living longer. However, screening and tests have declined—some say too much—as the field responded to claims of overtreatment. Today, the challenge is distinguishing small, low-risk cancers from those likely to metastasize. Doctors say that genomics tests, which look at the biology of a tumor, provide precious clues. The tests have been used extensively on breast cancer to determine which women can be spared chemotherapy. Several prostate-cancer genomics tests, including Prolaris and Decipher, have come on the market in recent years. Oncotype DX, made by Genomic Health, was launched in 2013. Its use isn't as widespread as the company's breast-cancer test, company officials say, but is growing. The various genomics tests, which have a list price between $3,800 and $5,000, generally are covered by Medicare and some private insurers. Results can prompt patients to change course radically. In the fall of 2016, Ken Huner scheduled surgery to have his prostate removed after learning he had low- to intermediate-risk cancer. Mr. Huner, a financial consultant from Milan, Mich., went for a second opinion. His new doctor, Todd Morgan, is a member of Music---Michigan Urological Surgery Improvement Collaborative---a group of urologists whose aims include curbing overtreatment. Dr. Morgan, a urologic oncologist at the University of Michigan, ordered a genomics test, Prolaris. Based on encouraging results, Dr. Morgan told Mr. Huner that without treatment he had only a 3% chance of dying over the next decade from prostate cancer. Mr. Huner canceled his surgery and ever since has been on active surveillance, the course Dr. Morgan suggested. For a man diagnosed with prostate cancer, "it is an incredible struggle if they are borderline" between low- and intermediate-risk cancer, Dr. Morgan says. "We need some type of tie-breaker." He sees genomics test results filling that role in some cases. 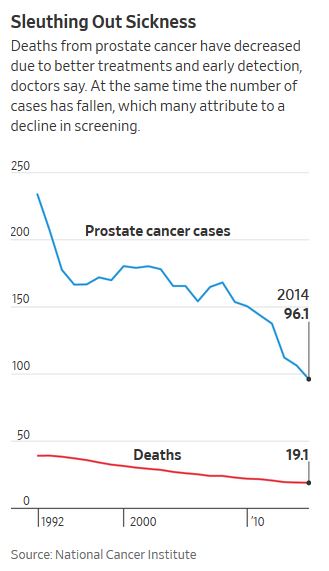 At the annual meeting of the American Urological Association in May, Dr. Morgan will unveil a study of how genomic testing influenced treatment decisions. His team looked at 3,966 Michigan men diagnosed with early-stage prostate cancer, and found that those "who underwent [genomics] testing were significantly more likely to undergo surveillance," Dr. Morgan says. Among patients with low-risk or low-to-intermediate-risk cancer who scored favorably on the genomics test, 78% chose active surveillance compared with 57% of men who didn't take the test. Other doctors are more guarded. "No one test is that good," says Eliezer Van Allen, a medical oncologist at Dana-Farber Cancer Institute who runs a research laboratory on genomics. "All our patients are asking us to do the impossible, which is to see the future," he says. "The reality is filled with uncertainty." The prostate-cancer genomics test is still fairly new, he says, and there isn't enough data on it. In addition, a favorable result one day doesn't mean a patient is home free forever. The genomics tests "are useful...in the moment," says Eric Klein, a Cleveland Clinic urologist who was involved in early studies of Oncotype DX. He sees them answering the question: Does this patient have a cancer that needs treatment? However, "that does not mean he won't need treatment in the future," he says. Dr. Klein, chairman of the Glickman Urological and Kidney Institute, is on an American Society of Clinical Oncology panel considering guidelines for genomics testing of prostate cancer. He has been a paid consultant for the makers of Oncotype DX and Decipher, but has no financial interest in the companies. Peter Carroll, a surgeon and the chairman of urology at UCSF Health in San Francisco, runs an active surveillance program of prostate-cancer patients, some of whom have been followed for years. Genomics testing "tells you which patients aren't likely to progress and which are harboring disease which you should not be watching—you should be treating," he says. Albert "Tony" Cellini had a taste of both the joy and heartbreak that the tests can trigger. Mr. Cellini, 67, a retired equities trader in San Francisco, was diagnosed with prostate cancer in 2013. He had his first genomics test in 2015, which—along with other aspects of his disease—suggested he could continue active surveillance. Last year, he had another biopsy—and genomics test—which showed a dimmer picture. Dr. Carroll's conclusion: "Treatment rather than surveillance may be in order." Mr. Cellini had surgery in January. He has been suffering some side effects but is grateful for nearly five years without treatment. "My cousin asked me, 'If you had to do it all over again, would you do active surveillance?' and I said, 'Absolutely.' " Over the weekend, Mr. Michel received disturbing news. Dr. Katz, his urologist, was troubled by Mr. Michel's recent MRI and says it may be time to step up from active surveillance to treatment, preferably radiation. It's disappointing to Mr. Michel, who says, "I was looking for a five-year, six-year run" of surveillance. Copyright ©2018 Dow Jones & Company, Inc. |
Return to PC Home Page